

Introduction
Anemia Mukt Bharat (AMB) is a flagship programme of Ministry of Health and Family Welfare (MoHFW) under POSHAN Abhiyaan. The programme aims at reducing anemia through a life cycle approach.
Organizing Test-Treat-Talk (T3) anemia camps (henceforth called T3 camps) is an integral component of AMB’s demand generation, social and mass mobilization strategy. Each T3 camp is one-day long, held at a fixed site and fixed time and caters to an average of 500 beneficiaries. Beneficiaries can be of all or a specific group such as pregnant women, adolescents, etc., depending on the site of camp. A typical T3 camp consist of three steps; Test for anemia using a digital hemoglobinometer (invasive); Treat with iron-folic acid (IFA) tablets and referral; and Talk or counsel beneficiaries on iron, protein and vitamin C rich foods and healthy lifestyle measures.
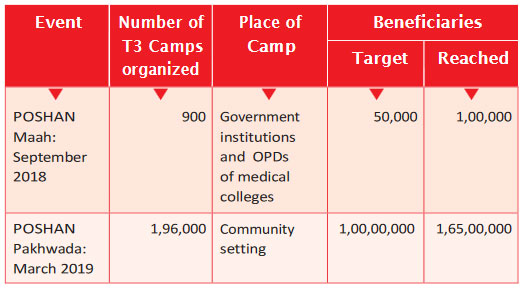
The Jan Andolan Dashboard Data – (Table 1) shows thatduring POSHAN Maah (September 2018) and POSHAN Pakhwada (March 2019), several States in collaboration with medical colleges, academic institutions, development partners, etc. T3 camps which together reached out to over 1.75 crore people. As shown in Table 1, the POSHAN Pakhwada showed a huge increase in the number of beneficiaries covered, jumping from 1 lakh during POSHAN Maah in September 2018 to 1.65 crore during POSHAN Pakhwada in March 2019. This demonstrates the community’s acceptance and programmatic feasibility of scaling-up the T3 approach.
Table 1: Coverage of T3 camps in POSHAN Maah (September
2018) and POSHAN Pakhwada (March 2019)
Target for POSHAN Maah, September 2019: Anchored in the success of the T3 approach, the States and union territories (UTs) for the upcoming round of POSHAN Maah 2019 should set an ambitious target to reach as many people as possible. During this POSHAN Maah, States and UTs should focus on setting up of T3 camps across all government and government-aided schools and colleges of the country in addition to setting up T3 camps at community level such as VHND, AWC, Health facilities, Railway
Stations, Bus stands and Weekly markets etc.
It is envisaged that the September 2019 T3 camp in schools and colleges will encourage children to inculcate healthy dietary habits. This will go a long way towards improving their cognitive potential and enhancing the physical and mental capacity of the young generation. It will also generate awareness on anemia among the masses.
This guidance note is intended to support State Programme Managers in training and orienting their district and block teams in:
i. How to plan and organize a T3 camp
ii. How to monitor and report T3 camp activities
Benefits of organizing a T3 camp
Organizing a T3 camp would have many benefits, such as:
- Creating a buzz and visibility about the anemia and the Anemia Mukt Bharat programme
- Providing personalized treatment and counselling based on an individual’s hemoglobin level/anemia level
- Serving as a gateway to promote nutrition messages on healthy diets (iron, protein and vitamin C rich foods, fortified
foods and double fortified salt), do’s and don’ts for anemia and iron rich food recipes
Preparations needed for organizing a T3 camp
There are three critical steps that must be followed when organizing a T3 camp:
A) Planning:
- The State NHM–AMB nodal officer may call for a planning and sensitization meeting with the district nodal/RCH officers for AMB and officers from the Department of Education, Department of Panchayati Raj, partner medical and nutrition colleges and development partners at NHM Office (Sample agenda at Annexure 1)
- The meeting should discuss the date, venue, time, work allocation, social mobilization, logistics, checklist to organize a camp ; how to implement, record and report (please see Annexure 6)
- A joint letter for implementing T3 camps should be issued for respective programme management units (Health and Education)
- The meeting should be held at least 20 days before celebrating POSHAN Maah (preferably in the second week of August).
- At the district level and block level, directives should be sent to the frontline workers to plan and organize activities to inform the community about the upcoming T3 camp.
- In order to leverage the micro plan and logistics required, the day on which IFA tablets are administered in schools and colleges may be fixed for organizing theT3 camps.
- The camps may be organized so as to encourage participation of the general population staying in the vicinity of the venue. This would improve the reach of awareness generation activities on anemia prevention and control.
- Utmost care should be taken for disposal of biomedical waste
generated at the camp site. The school/college authority should coordinate with the nearest PHC/CHC medical officer for proper disposal of waste.
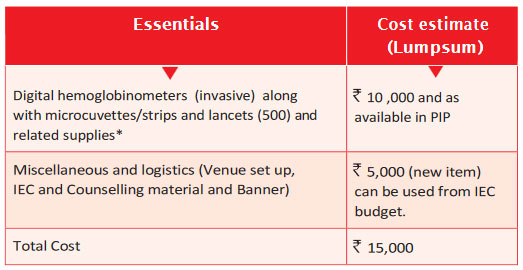
Table 2: Estimated Budget for one T3 camp
B) Sensitization meeting (at State and district levels):
Salient points to be discussed during the meeting:
- Target beneficiaries: Children (5–9 years) and adolescents (10–19 years) in school and colleges. Teachers, parents and local population will also be part of the T3 camp.
- Number of camps: It is suggested that at least 50 camps
per district may be organized in the premises of government
and government–aided schools and colleges. - Human resource: One ANM/lab technician, one medical
officer/resident/intern, two dieticians/nutritionists to counsel
the target beneficiaries.
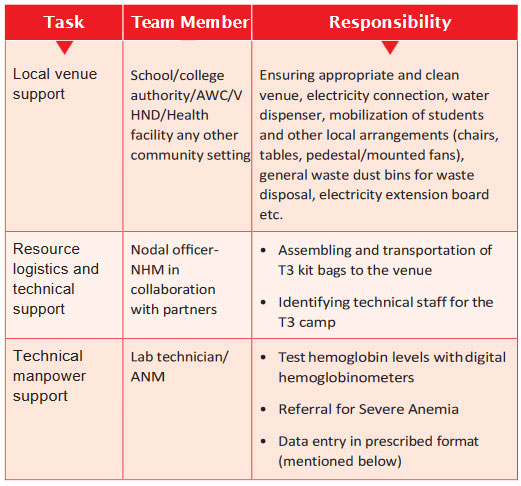
Table 3: Brief on job responsibilities of each team member in a T3 camp:
- Ready to print samples of Banner and IEC material is available for free download at www.anemiamuktbharat.info/resources/ T3camp
- The respective State NHM team may request the departmentn of pediatrics and preventive and social medicine at the partner medical colleges to provide necessary manpower and logistics support
- To fulfil the requirement of Dieticians/Nutritionists, the State may contact Home science/agriculture/relevant allied academic institutions for volunteer dietary counselling support during the camp.
C) Joint directives followed by video conference (VC) with district teams:
A joint letter co–signed with Department of Health and Education explaining the date, purpose and process along with guidance note to be shared (sample letter in Annexure 5)
Implementation of T3 camp
- A day–long camp during school hours (preferably 8.30 a.m. to 1 p.m.) shall be held in the premises (auditorium, hall, meeting rooms, etc.) of government and government–aided schools and colleges.
- Setting–up of the camp must be ensured one day (preferably) prior of holding the camp.
- Each camp will be manned by 4–5 people including one medical doctor/resident doctor/intern, one ANM and two nutritionists/dieticians.
- School/college authorities must take responsibility for local arrangements and logistics support at the venue.
- In addition to hemoglobin testing, initiation of treatment of identified anemic children, counselling on iron, protein, vitamin C rich and fortified foods, do’s and don’ts to improve hemoglobin levels and information, education and communication materials should also be distributed to the participants.
- Display of IFA tablets at the camp site should be ensured from the existing NHM resources. Cases identified as severely anemic should be referred to the nearest government health facility for further treatment by the medical officer.
- Demonstration of recipes/display of IEC materials on locally available homemade food rich in iron, protein and vitamin C. Pamphlets/leaflets on the recipes may be distributed. To improve footfalls, attractive selfie booths should be set up where people with normal Hb levels can be photographed holding placards displaying messages such as “Solid Body Smart Mind – I am Anemia–free”, “Sahi Poshan Desh Roshan”, “Solid Hai Bharat – Anemia Mukt Bharat.“ etc. Sample banner is at Annexure 4.
- Pictures and short videos from the camp should be uploaded on social media platforms (Twitter/Facebook) and also on POSHAN Abhiyaan: Jan Andolan Dashboard to create awareness on anemia
Procedure at T3 camp
Testing for anemia
Hemoglobin estimation using digital hemoglobinometer
Checklist for estimation of hemoglobin using digital hemoglobinometers:
- Digital hemoglobinometers with batteries or charger
- Microcuvettes or strips
- Lancets
- Alcohol swab/spirit cotton
- Non–sterile gloves
- Tissue paper/cotton
- Biomedical waste container (puncture–proof) and biomedical waste disposal bag to dispose the used lancets, microcuvettes / strips and cotton/alcohol swabs
A. Collection of capillary blood sample
I. Wear non–sterile gloves on both of your hands.
II. Choose the third (middle) or fourth (ring) finger of the subject’s
non–dominant hand for the finger prick.
Precautions:
- Avoid the thumb and little finger.
- Avoid fingers with thick calluses.
- Avoid fingers with tight rings as they may constrict blood flow.

III. Ask the subject to rub their hands to promote blood flow.
IV. Wipe the fingertip with the alcohol swab/spirit cotton and let it
air dry completely.
Precautions:
- Do not blow on the finger to dry the alcohol.
- Do not wipe off the alcohol
- Do not perform the finger prick until alcohol is completely
evaporated.
V. Hold the finger firmly just below the centre of the fingertip
VI. Press and trigger the lancet flat and firmly against the finger at
the puncture sites away from the midline as shown in Figure 4
VII. Discard the lancet in a biohazard container.
VIII. Release pressure and allow a full drop of blood to collect on the
finger.
IX. Once a drop of blood has collected on the finger, use a cotton or
tissue to wipe away the first drop of blood.
X. Use the second or third drop of blood for estimation of hemoglobin.
XI. Discard the cotton/tissue in a biohazard container.
B. Estimation of hemoglobin using digital hemoglobinometers
a) Testing hemoglobin using microcuvette
- Turn “ON” the meter. After the monitor shows three dashes, pull the cuvette holder in its loading position.
- Fill the microcuvette in one continuous process. The correct amount of blood (10 μl) is drawn into the microcuvette. The microcuvette should be completely filled
- Wipe away any excess blood on the outside of the microcuvette tip
- Check for air bubbles in the filled microcuvette. If present,
use a new microcuvette - Place the filled microcuvette in the cuvette holder (within 40 seconds after filling the cuvette)
- Push the cuvette holder to its measuring position Read and record the result. Remove and discard the microcuvette in an appropriate biohazard container. Push the cuvette holder back into the instrument
b) Testing of hemoglobin usingstrip
- Turn “ON” the meter. The system undergoes an autocheck and auto–calibration after which the battery level, date, time and strip’s batch code are displayed within 2 seconds
- Enter the code mentioned on the strip bottle
- The meter will flash ‘STRIP’ symbol on the display. Insert a fresh test strip into the meter with the arrows on the strip facing up and pointing towards the display
- Ensure the correct positioning of the strip with the guiding V notch
- The meter will flash ‘DROP’ symbol on the display. Allow the second drop of the blood to fall to completely cover the white coloured test area.
- Read and record the result
- Remove the used test strip from the meter and dispose in an
appropriate biohazard container
Treatment for Anemia
Classification of anemia based on hemoglobin level
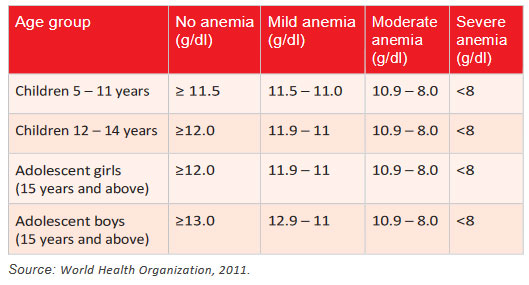
19Guidance Note for State Programme Managers Treatment of anemia for children and adolescents (aged 5–19 years) attending T3 camps
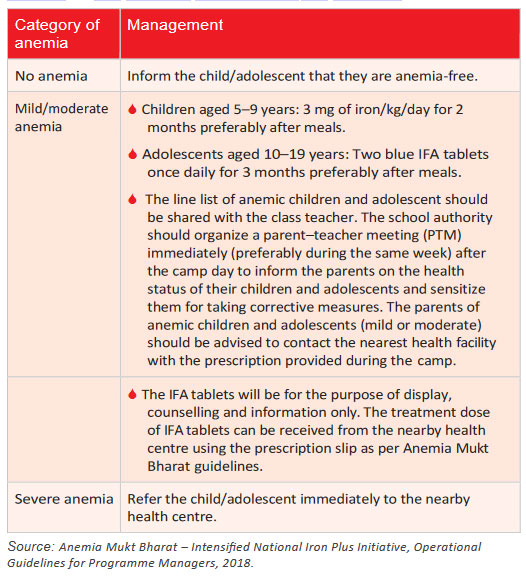
Key notes for T3 camps at schools
- At all schools, the class teachers should accompany their respective class children during the testing for anemia, treatment and talk/dietary counselling during the camps.
- The prescription slip should be to given the respective class teachers.
- A parent–teacher meeting should be held immediately (preferably in the same week) after the T3 camps.
- Teachers need to hand over the prescription slips to the parents and guide them for further follow–up in the referred health centres.
- The IFA tablets will be only for display purpose to generate awareness on the availability of treatment option at the nearest health facility.
- During the meeting, parents have to be informed on iron–, protein– and vitamin C–rich foods, dos and don’ts during consumption of IFA tablets.
- Teachers should also inform the parents regarding the need for follow–up visit at the nearby health centre after the completion of treatment to assess the improvement in hemoglobin.
- The WIFS nodal teacher of the school will be coordinating all
these activities.
Talk for Anemia
- Provide one–to–one counselling.
- Use the dietary counselling materials provided in the T3 kit bag
during the counselling. - Provide counselling on iron, protein and vitamin C rich food
intake. - Provide information on iron rich food recipes.
- Explain the dos and don’ts for anemia.
- Provide dietary counselling to all anemic children.